To what extent do people in different parts of the world face the same health risks, and why?
Different disease seem to appear with different ages with general environment. Apparently the health risks are depend on what kind of disease one is posing out. It does not seem to be completely comparable, for people to compare the risks of health in different regions of the world. I can argue that these diseases, such as heart disease, cancers, HIV/AIDS, can be seen as inevitable for different levels or ages of life and living styles, thus everyone has the same health risks. However, if I take human rights into account, it will be obvious that health inequality is the truth. Poverty is a major problem of causing the higher health risks. There are different risks factors, such as education, social and economic positions. These factors make people of lower positions more vulnerable when facing health issues, as a result they get sicker and die sooner.
Education wise, the basic acknowledgement directly affect a region of health care. Just look at the fact that education improve poorer-countries' health care, it is obvious that education is essential as the very first step. For example Ethiopian health care begins with hospitals, with more than 80% of the people live in rural area. The health care center has labs that can diagnose parasites. A boy who was being tested with malaria with a pin-prick test that has dramatically improved diagnose and treatment. When he was founded positive, the health extension worker can begin treatment immediately. Another little child was extremely sick with diarrhea, which is the leading cause of death in Ethiopia although it is always survivable when children can stay hydrated. Eventually the boy went home with solution that might well have saved his life. There are women who volunteer to be part of the infant care center, which one of them is educated to grade 10 and she works on organizing the case reports and different diseases in her area and that is how the medical care in Ethiopia trying to improve. Another interesting fact is that, because the medical care is now required to have birth records, the mothers in Ethiopia happen to name their children right after their births instead of naming after about their births of six months or so. In this case, it includes how a better health care support from governments and other organization with budgets and education greatly contribute to a whole region's health services.
Economically advantaged people have obviously more access to both preventive care and curative care. While the worst thing is that poorer countries cannot really afford the costs, it is also important to recognize that even in developed countries, there are people in lower social status struggling with spending money on health care or other necessities such as shelter and nutriments. It is ironic that people get to choose whether they want to spend their limited amount of budget on the necessities they need or health services that they also need. Another thing that is happening in America is that only people who work in big corporation, are old or students, have the guarantee of health care, essentially it causes people to either work in big corporation or stay as students. Big corporations are required to accompany with health insurance company thus the workers are guaranteed to have health care. People who are able to afford the costs of preventive care and curative care have less risks than those who are not.
Every-time when someone engage with drugs, one takes a risk; just like exercise can lead to injuries. Drugs have side effects too. Especially for those who have less access to health care, if their bodies are resistance to treatments, it is much harder for them to get further help with such resistance.
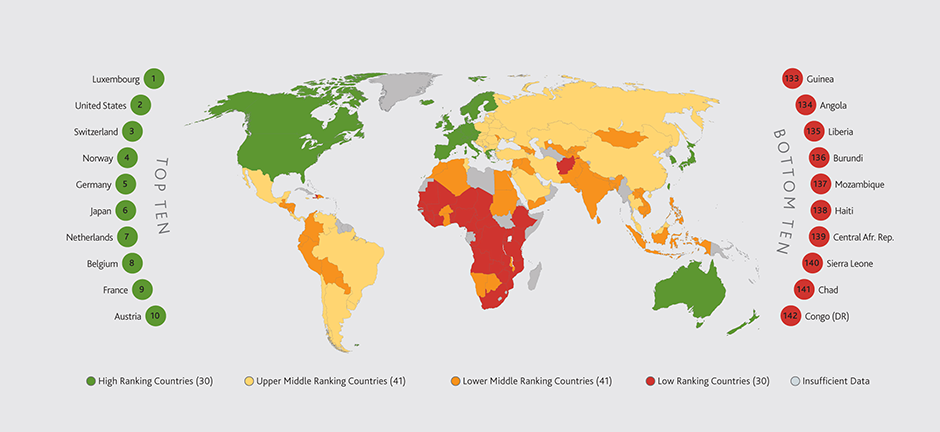
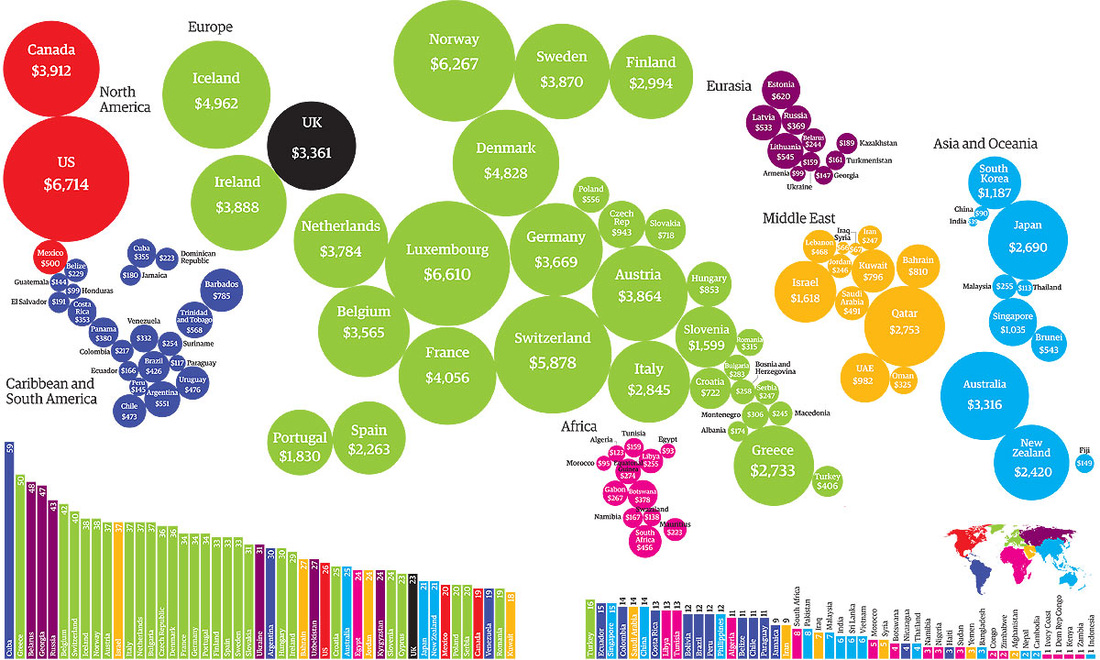
There are several cool maps show how NCDs, noncommunicable diseases - the leading causes of death worldwide, contribute to poverty and how poverty contributes NCDs. It begins with globalization, urbanization and population aging. Then all of them increased exposure to common minor change of risk factors such as unhealthy diets, physical inactivity, tobacco use, harmful use of alcohol. Subsequently the factors above lead to the loss of household income from unhealthy behaviors and noncommunicable diseases of which include cardiovascular diseases, cancers, diabetes, and chronic respiratory diseases. Then the noncommunicable diseases lead to ,first, more loss of household income from poor physical status and premature death; second, limited access to effective and equitable health-care services, which respond to the need of people which noncommunicable diseases, eventually lead to the loss of household income from high cost of health care. All of the loss of household income have contributed to poverty at household level that leads to create countries with populations in low- and middle-income.
Overall, health care is directly related to the economic status one has, which perfectly differentiate the risks within different part of the world.
Different disease seem to appear with different ages with general environment. Apparently the health risks are depend on what kind of disease one is posing out. It does not seem to be completely comparable, for people to compare the risks of health in different regions of the world. I can argue that these diseases, such as heart disease, cancers, HIV/AIDS, can be seen as inevitable for different levels or ages of life and living styles, thus everyone has the same health risks. However, if I take human rights into account, it will be obvious that health inequality is the truth. Poverty is a major problem of causing the higher health risks. There are different risks factors, such as education, social and economic positions. These factors make people of lower positions more vulnerable when facing health issues, as a result they get sicker and die sooner.
Education wise, the basic acknowledgement directly affect a region of health care. Just look at the fact that education improve poorer-countries' health care, it is obvious that education is essential as the very first step. For example Ethiopian health care begins with hospitals, with more than 80% of the people live in rural area. The health care center has labs that can diagnose parasites. A boy who was being tested with malaria with a pin-prick test that has dramatically improved diagnose and treatment. When he was founded positive, the health extension worker can begin treatment immediately. Another little child was extremely sick with diarrhea, which is the leading cause of death in Ethiopia although it is always survivable when children can stay hydrated. Eventually the boy went home with solution that might well have saved his life. There are women who volunteer to be part of the infant care center, which one of them is educated to grade 10 and she works on organizing the case reports and different diseases in her area and that is how the medical care in Ethiopia trying to improve. Another interesting fact is that, because the medical care is now required to have birth records, the mothers in Ethiopia happen to name their children right after their births instead of naming after about their births of six months or so. In this case, it includes how a better health care support from governments and other organization with budgets and education greatly contribute to a whole region's health services.
Economically advantaged people have obviously more access to both preventive care and curative care. While the worst thing is that poorer countries cannot really afford the costs, it is also important to recognize that even in developed countries, there are people in lower social status struggling with spending money on health care or other necessities such as shelter and nutriments. It is ironic that people get to choose whether they want to spend their limited amount of budget on the necessities they need or health services that they also need. Another thing that is happening in America is that only people who work in big corporation, are old or students, have the guarantee of health care, essentially it causes people to either work in big corporation or stay as students. Big corporations are required to accompany with health insurance company thus the workers are guaranteed to have health care. People who are able to afford the costs of preventive care and curative care have less risks than those who are not.
Every-time when someone engage with drugs, one takes a risk; just like exercise can lead to injuries. Drugs have side effects too. Especially for those who have less access to health care, if their bodies are resistance to treatments, it is much harder for them to get further help with such resistance.
There are several cool maps show how NCDs, noncommunicable diseases - the leading causes of death worldwide, contribute to poverty and how poverty contributes NCDs. It begins with globalization, urbanization and population aging. Then all of them increased exposure to common minor change of risk factors such as unhealthy diets, physical inactivity, tobacco use, harmful use of alcohol. Subsequently the factors above lead to the loss of household income from unhealthy behaviors and noncommunicable diseases of which include cardiovascular diseases, cancers, diabetes, and chronic respiratory diseases. Then the noncommunicable diseases lead to ,first, more loss of household income from poor physical status and premature death; second, limited access to effective and equitable health-care services, which respond to the need of people which noncommunicable diseases, eventually lead to the loss of household income from high cost of health care. All of the loss of household income have contributed to poverty at household level that leads to create countries with populations in low- and middle-income.
Overall, health care is directly related to the economic status one has, which perfectly differentiate the risks within different part of the world.
 RSS Feed
RSS Feed